
The Ebola virus is an enveloped virus, the class most susceptible to germicidal UV-C light. No published study has irradiated live Ebola at 254 nm on a surface, so the case rests on read-across from other enveloped viruses and CDC guidance. UV-C works as a no-touch adjunct after manual cleaning, never a replacement.
When a suspected Ebola case moves through your unit, the room it leaves behind becomes part of the problem you have to solve. The 2026 Ebola outbreak has put that question back in front of infection prevention teams worldwide: once the patient is moved, how do you make the environment safe for the next one? This article looks at what the published evidence actually says about UV-C disinfection and the Ebola virus, how long the virus survives on hospital surfaces, and where a no-touch UV-C step fits alongside the manual cleaning your team already does.
Why does the environment matter so much in this outbreak?
The 2026 outbreak is caused by Bundibugyo ebolavirus and is centred in the Democratic Republic of the Congo, with cases in Uganda. The World Health Organization declared it a Public Health Emergency of International Concern on 17 May 2026, and it has since become one of the largest Ebola outbreaks on record.1
One detail shapes everything that follows: the licensed Ebola vaccines and treatments were certified against the Zaire species, not Bundibugyo, so there is currently no approved vaccine or proven treatment for this strain.2 When pharmaceutical tools are limited, the weight shifts onto the measures that break transmission directly: early isolation, personal protective equipment, safe waste handling, and environmental cleaning and disinfection. The environment is not a footnote in Ebola care. It is a frontline.
That reality is not confined to the outbreak zone. Gulf health authorities have moved early: Saudi Arabia restricted travel and visas from affected countries and reinforced screening at points of entry, and the Public Health Authority (Weqaya) confirmed its surveillance system was ready to protect residents and pilgrims through the Hajj season.9 Preparedness now includes the question of what a hospital does with a room after a suspected case.
How long does the Ebola virus survive on hospital surfaces?
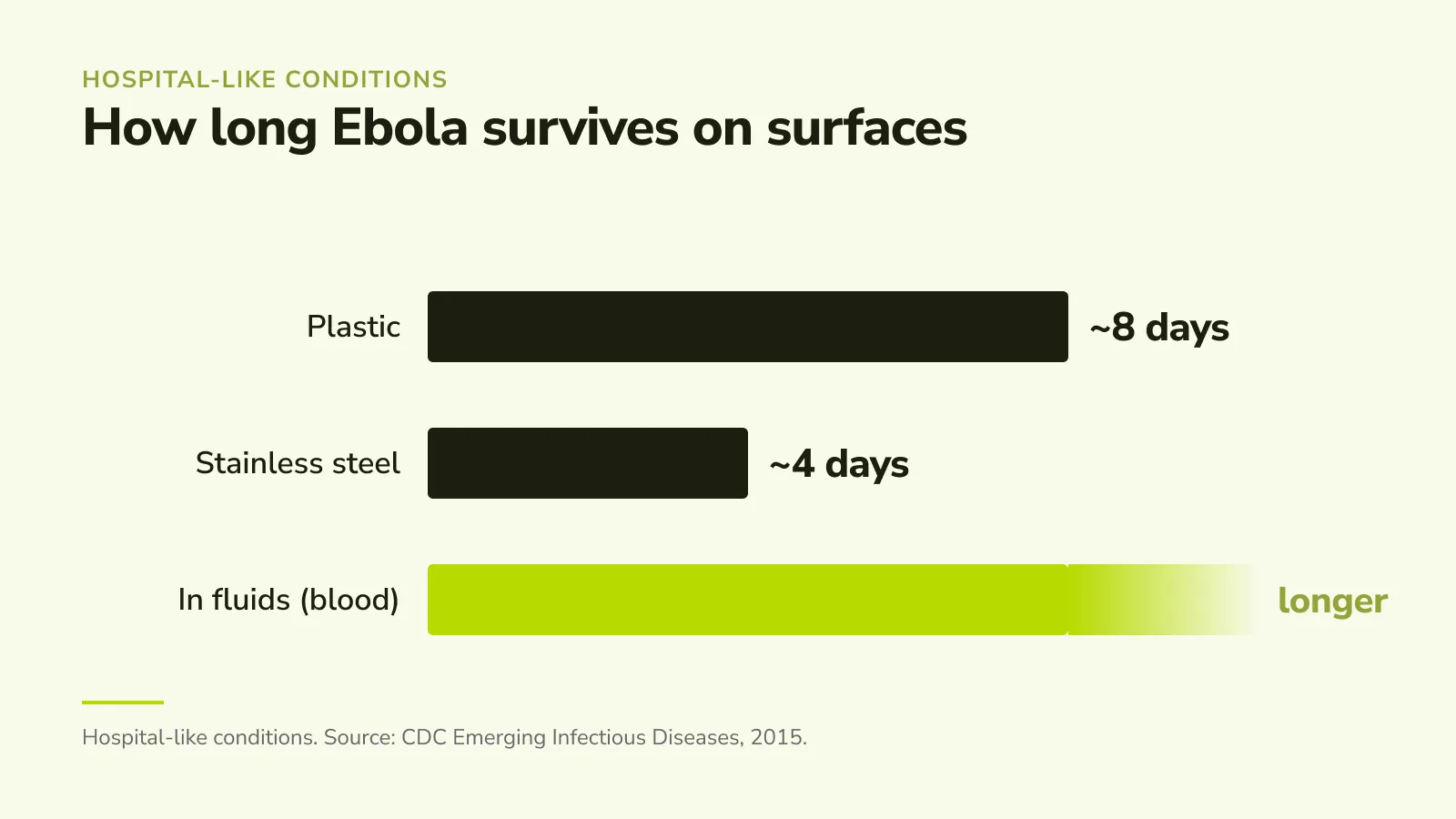
Under hospital-like conditions, the Ebola virus has been shown to remain viable for up to 8 days on plastic and about 4 days on stainless steel, and longer in liquids such as blood.4 Cooler, low-humidity indoor settings extend survival compared with hot, humid outdoor conditions.
This is the reason terminal disinfection carries weight. Ebola spreads primarily through direct contact with the bodily fluids of an infected person, but the surfaces those fluids reach — bed rails, over-bed tables, monitors, door handles — become a secondary reservoir. The longer the virus persists on a high-touch surface, the more that surface matters to the next patient and to the staff who enter the room.
Is the Ebola virus vulnerable to UV-C light?
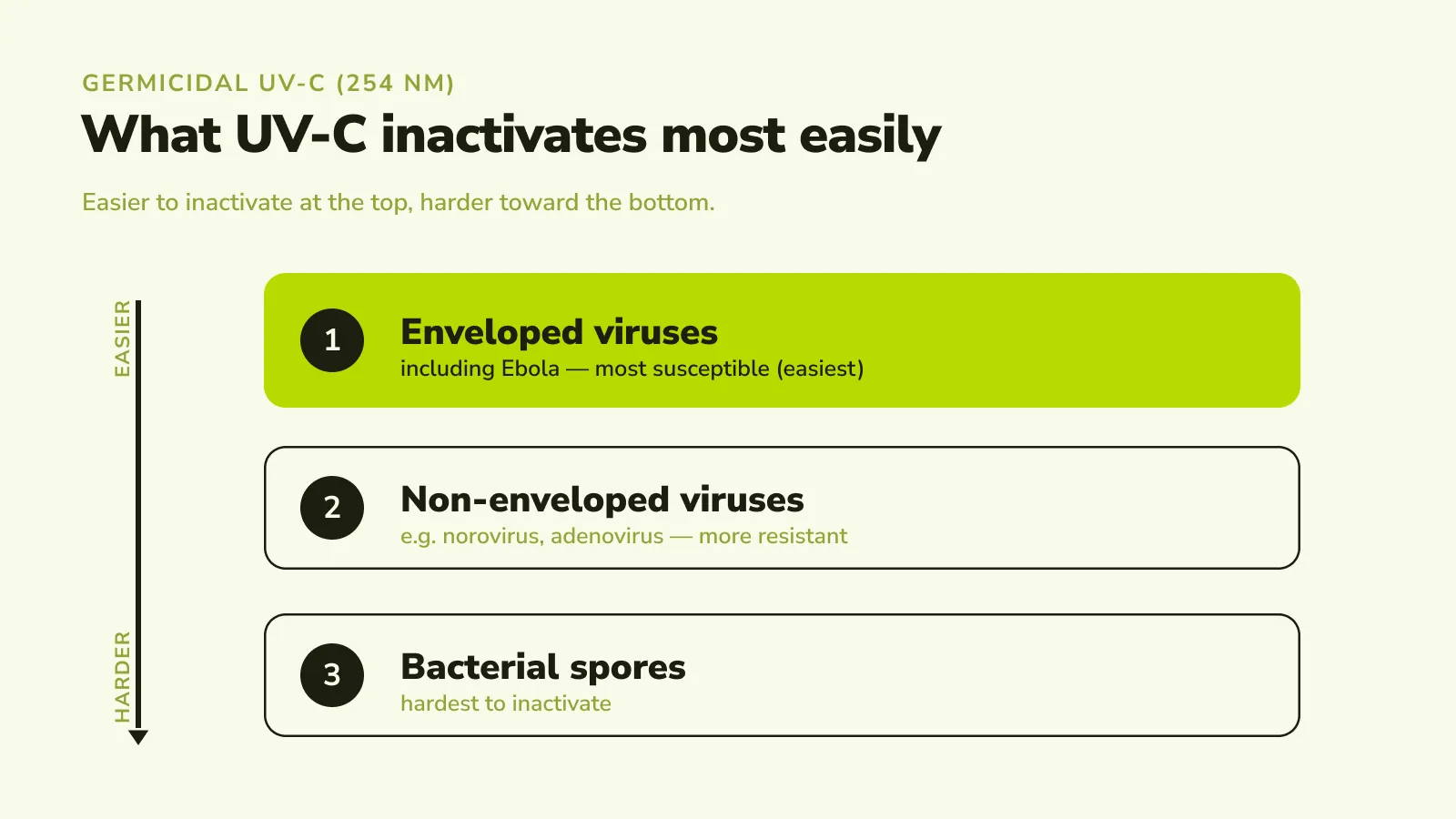
The Ebola virus is an enveloped, single-stranded RNA virus, and enveloped viruses are consistently the most susceptible class of microbes to germicidal UV-C (254 nm). Because live Ebola has not been irradiated at 254 nm on a surface in a published study, the expectation comes from read-across across enveloped viruses and from official guidance, rather than from direct Ebola data.
Two lines of evidence support this. First, the physical mechanism: UV-C at 254 nm damages the genetic material of a microbe so it can no longer replicate, and the fragile lipid envelope and RNA genome of viruses like Ebola offer little resistance. In controlled studies of the enveloped virus SARS-CoV-2, surface-dried virus was reduced by more than 6 log (a 99.9999% reduction) at a dose of about 3.5 mJ/cm² of 254 nm UV-C,5 and roughly 12.5 mJ/cm² achieved a 3-log reduction in suspension.6 Enveloped viruses reach these reductions at lower doses than hardier, non-enveloped viruses and bacterial spores.
Second, official guidance treats Ebola as an easy target for surface disinfection. The CDC states plainly that although no product carries a specific Ebola label claim, enveloped viruses such as Ebola are susceptible to a broad range of hospital disinfectants used to disinfect hard, non-porous surfaces.3 UV-C is one such no-touch surface-disinfection method, applied to the same hard, non-porous surfaces after they have been cleaned.
What we do not claim
Accuracy is the point of an article like this, so the limits belong in the open. No published study has measured 254 nm UV-C inactivation of live Ebola virus dried on a surface, so we do not present a specific Ebola log-reduction figure or state that UV-C "kills Ebola." UV-C is a no-touch adjunct for environmental surface disinfection. It is not high-level disinfection — a term reserved for reprocessing semi-critical medical devices — and it does not replace manual cleaning, PPE, isolation, or any other element of the IPC bundle. What the evidence supports is a reasoned expectation, grounded in the enveloped-virus class and in CDC guidance, that Ebola is well within reach of germicidal UV-C on a properly pre-cleaned surface.
Where does UV-C fit in the cleaning process?
WHO and CDC guidance for Ebola care puts environmental cleaning and disinfection among the core measures that reduce in-hospital transmission, alongside isolation, PPE, and safe waste handling.83 Manual cleaning does the essential first job: it removes visible soil and the bulk of contamination, which is what lets any disinfection step work. But manual cleaning depends on reaching every surface, every time, with the right contact time. High-touch points get missed, shadowed areas get skipped, and pressure on room turnover works against thoroughness.
A no-touch UV-C cycle is the layer that addresses that variability. After the room is manually cleaned, the emitter delivers a consistent, measured dose of 254 nm light to exposed surfaces, including the ones a rushed wipe-down can miss. For the general no-touch principle there is trial evidence in bacteria: adding automated UV to standard terminal cleaning was associated with roughly a 30% reduction in the acquisition of key multidrug-resistant organisms in a multi-centre randomised trial.7 That result is about bacteria, not Ebola, and we cite it only for the adjunct principle: UV-C catches what manual cleaning leaves behind.
UV-C vs manual cleaning: what does each one do?
| Comparison aspect | Manual cleaning (essential first step) | No-touch UV-C (adjunct, after cleaning) |
|---|---|---|
| Main job | Removes visible soil and bulk contamination | Delivers a measured germicidal dose to exposed surfaces |
| Reaches | Wherever the cloth reaches; depends on the person and the time available | Every surface in the light path, including easily missed high-touch points |
| Consistency | Varies with workload, training, and turnover pressure | The same documented cycle in every room |
| Chemical use | Required | None during the UV step |
| On its own | Can leave shadowed or skipped surfaces | Cannot remove soil; needs a clean surface to work |
| Together | The bulk removal that makes disinfection possible | The verification layer that closes the gaps |
The two are not alternatives. Manual cleaning makes the surface ready, and UV-C treats what remains.
What does this mean for hospitals and IPC teams?
For an infection prevention team, the outbreak reframes an existing question: is your environmental disinfection capacity part of your preparedness plan, or only your PPE and isolation? Readiness includes the room. In a high-consequence isolation setting, the value of a no-touch step is not only the added assurance on the surface. It is also that a robot, not a person, spends the cycle time in the contaminated space, which reduces staff exposure during terminal disinfection.
For leadership and accreditation leads, particularly across the Gulf, the case connects to standards you already answer to. A documented, repeatable disinfection cycle produces the kind of audit-ready evidence that JCI, CBAHI, and GAHAR surveyors look for under infection prevention and facility-safety requirements. Preparedness that can be shown, per room and per cycle, is preparedness a board and a surveyor can both trust. Outbreaks test not only healthcare systems but the environments that support them, and the environment is something a hospital can plan for in advance.
How does the ROZOR Disinfection Robot support your team?
The ROZOR Disinfection Robot is built for exactly this layer: an autonomous, mapped 254 nm UV-C cycle that runs after your EVS team has cleaned the room, and logs each cycle for your records. It does not replace your cleaners or your protocol. It takes the repeatable, higher-exposure task off people and performs it the same way every time, so your team is freed to focus where their judgment matters most. In an outbreak, that combination — human cleaning plus consistent no-touch disinfection with a documented trail — is what turns a difficult room turnover into a reliable one.
If you are reviewing your environmental disinfection readiness, we are glad to walk through how a validated UV-C step fits your existing bundle.
Frequently asked questions
Does UV-C kill the Ebola virus?
The Ebola virus is an enveloped virus, the class most susceptible to germicidal UV-C. No published study has irradiated live Ebola at 254 nm on a surface, so a specific kill figure cannot be stated. Based on read-across from other enveloped viruses and CDC guidance, Ebola is expected to be highly susceptible to UV-C on a pre-cleaned surface.
How long does Ebola survive on hospital surfaces?
Under hospital-like conditions, studies have shown the Ebola virus remaining viable for up to about 8 days on plastic and around 4 days on stainless steel, and longer in liquids such as blood. Cooler, drier indoor conditions extend survival compared with hot, humid outdoor settings.
Can UV-C replace manual cleaning for Ebola?
No. UV-C is a no-touch adjunct, not a replacement. Manual cleaning removes the visible soil and bulk contamination that any disinfection step depends on. UV-C is applied afterwards to deliver a consistent germicidal dose to the surfaces that cleaning may miss. Both steps are needed.
Is UV-C the same as high-level disinfection?
No. High-level disinfection is a specific term for reprocessing semi-critical medical devices. UV-C room disinfection is environmental surface disinfection: an adjunct to terminal cleaning of the patient environment, not a device-reprocessing method.
Why does the environment matter so much in this outbreak?
The 2026 strain (Bundibugyo) has no approved vaccine or proven treatment, so measures that break transmission directly carry more weight. Because the virus can persist on high-touch surfaces for days, thorough environmental cleaning and disinfection is one of the core defences named by WHO and CDC.
Sources
- WHO. Ebola disease outbreak news and PHEIC declaration, 2026. https://www.who.int/emergencies/disease-outbreak-news
- CDC. 2026 Ebola outbreak situation summary. https://www.cdc.gov/ebola/situation-summary/index.html
- CDC. Interim guidance for environmental infection control in hospitals (viral hemorrhagic fevers). https://www.cdc.gov/viral-hemorrhagic-fevers/hcp/infection-control/environmental-infection-control-hospitals.html
- Fischer R. et al. "Ebola Virus Stability on Surfaces and in Fluids in Simulated Outbreak Environments." Emerging Infectious Diseases (CDC), 2015. https://wwwnc.cdc.gov/eid/article/21/7/15-0253_article
- Gidari A. et al. "SARS-CoV-2 Survival on Surfaces and the Effect of UV-C Light." Viruses, 2021. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8532508/
- "Systematic evaluating and modeling of SARS-CoV-2 UVC disinfection." Scientific Reports, 2022. https://www.nature.com/articles/s41598-022-09930-2
- Anderson D.J. et al. "Enhanced terminal room disinfection and acquisition of multidrug-resistant organisms (BETR-D)." The Lancet, 2017. https://pubmed.ncbi.nlm.nih.gov/28104287/
- WHO. Infection prevention and control guideline for Ebola and Marburg diseases. https://iris.who.int/
- Saudi public-health readiness coverage (Public Health Authority, Weqaya), 2026. Arab News; Saudi Gazette. https://www.arabnews.com/